“In three words I can sum up everything I’ve learned about life: it goes on.”
― Robert Frost
As I continue on my life journey and meet or talk with other prostate cancer patients, including those who’ve been newly diagnosed, I remind myself of how grateful I am that, to date, I have low-grade PCa, and am on an AS protocol. While anxiety creeps in when I’m awaiting the results of an MRI or biopsy, I wake up in the morning increasingly focused on how I can be creative and make the most of my day. I am keenly aware of men with more aggressive cancer who juggle treatments with different outcomes.
For now, I find fulfillment in listening to newly diagnosed and AS patient stories and questions, keeping up with the latest studies, and discovering new research outlets. And again, while I do not dispense medical advice, I concentrate on how I can provide reliable resources to men who may just need a guide that will empower them to make decisions with their doctors and specialists.
And, at the risk of repeating myself with statements from other posts, I always encourage patients to seek out second or even third opinions (should they need to break a tie!) if the decision involves a test or procedure. And I try to remember to impart a mantra that:
Being Alive, one day at a time, is a gift.

I do have some good news to report. At the end of my last Blog (#2), I spoke of my plan to have a transperineal biopsy at Brigham Women's Faulkner Hospital in Boston. Through contact I made with Adam Kibel, MD, Chief of Urology at Brigham, he referred me to Brigham urologist James Rosoff, MD. I had my confirming TP MRI-guided in-bore biopsy at Brigham four years ago, reporting nine benign samples – after which I could officially continue my AS. This time, I could have repeated an in-bore transperineal biopsy (inside the MRI tube). The in-bore technique has long been a gold standard as the medical specialist can see any suspicious areas the MRI picks up. However, my urologist does not perform in-bore biopsies but would have been happy for me to revisit with an interventional radiologist who had conducted my confirming biopsy four years earlier
I double-checked with Dr. Kemal Tuncali at Brigham, who elaborated on elements of the in-bore biopsy. However, he didn't have the newest transperineal equipment – the Precision Point System. (<---recommended reading). Given what I knew about Precision Point – specifically that other centers such as Johns Hopkins uses the system - I decided to go with a TP MR-Guided/fusion biopsy this go-around. Again, I had an MRI report graded Pirads-4 with a "stable" lesion. In a telehealth appointment, my doctor and I discussed what he would target and explained the fusion process at length. While I could have had the biopsy in his office with a local anesthetic, I chose to have a general anesthetic which moved my procedure to the hospital. A quick note about general anesthesia: one doctor on my team advised me of recent studies that general anesthesia carries a risk for older adults in memory loss. I looked up several studies – you can read one here – and I found that they were inconclusive. Everything with Prostate Cancer carries risk. Put that in your file. I have found that I have had to make many decisions based on risk assessment. They include uses of gadolinium contrast for imaging, the antibiotic ciprofloxacin, and risks of infection in transrectal vs. transperineal biopsies. Only with the latter issue is definitive science that backs up the claim that transperineal biopsies are less riskier for infection or sepsis. Although I cited it in my last Blog, read this article by Jeremy Grummet and others as to why transperineal biopsies are now considered the standard over TRUS biopsies. There is an effort to lobby the American Urological Association to add it to their guidelines in 2023. Arvin George, MD, in Michigan, is an excellent source of information about transperineal biopsies, as well as Michael Gorin, MD, and Australian Jeremy Grummet, MD(among others). Look for my Transperineal Analysis soon, including interviews with expert knowledge of the procedure.
Did I say that I consider Brigham a significant center of excellence among several throughout the US? If I didn’t, let me iterate it now. They have a stellar staff and are thorough in gathering pertinent patient information and informing patients of prerequisites before a biopsy.
THE RESULTS ARE IN…!

The pathology report arrived less than a week after my procedure, and I reviewed the results with Dr. Rosoff. The lab analyzed the samples the doctor had taken: all benign with three Gleason Grade 6s (3+3), which allowed me back on the yellow brick road of Active Surveillance and my monitoring protocol.

I felt relieved that pathologists did not find any aggressive tumors. It is a familiar feeling among all patients on the AS protocol when pathology results do not change their status of harboring low or intermediate favorable risk PCa.
MOVING RIGHT ALONG ….BIOMARKERS & SCREENING
(This section is for those on Active Surveillance, the newly diagnosed, and for those men who have not yet begun screening for Prostate Cancer , so PLEASE SHARE and copy and paste the link for your friends or loved ones: https://www.ASProstateCancer.blog
For those who wish to know – before you screen for Prostate Cancer – there are standard initial screening procedures. They include what age men should begin the screening process, and these guidelines are available from centers of excellence and scientific studies. Watch this short video from the CDC. Although it is a bit dated, it contains some good information - below I update the numbers for you. You’ll also see below a second reference on screening recommendations from Johns Hopkins.
Since this CDC video, many in the prostate cancer medical community are recommending screening at earlier ages, especially for men with family history or positive genetic test results, and African American men. It is also a fact that, although it is rare, there are men as young as 35 (and perhaps younger) who begin to develop issues with their prostate.
I have previously emphasized the importance of shared decision-making (SDM) among patients, doctors, and caregivers. SDM begins at screening, and the following link is from the annual AUA meeting in 2022, surveying disparities in the shared decision-making process.
It's an excellent informative article for your research toolbox.
Again, while I do not provide medical advice, first questions about PCa screening are usually discussed with a urologist you trust. If you do not have one, you may want to ask your primary care provider and seek out a couple of other recommendations in your community. You can always have a consultation with one and get a second opinion from another. Suppose you belong to one medical center where all the medical staff knows each other. In that case, you may want to consider finding your second opinion from outside that medical enclave. Although this is not absolute, doctors and specialists affiliated with one practice tend to stick together and not contradict their colleagues.
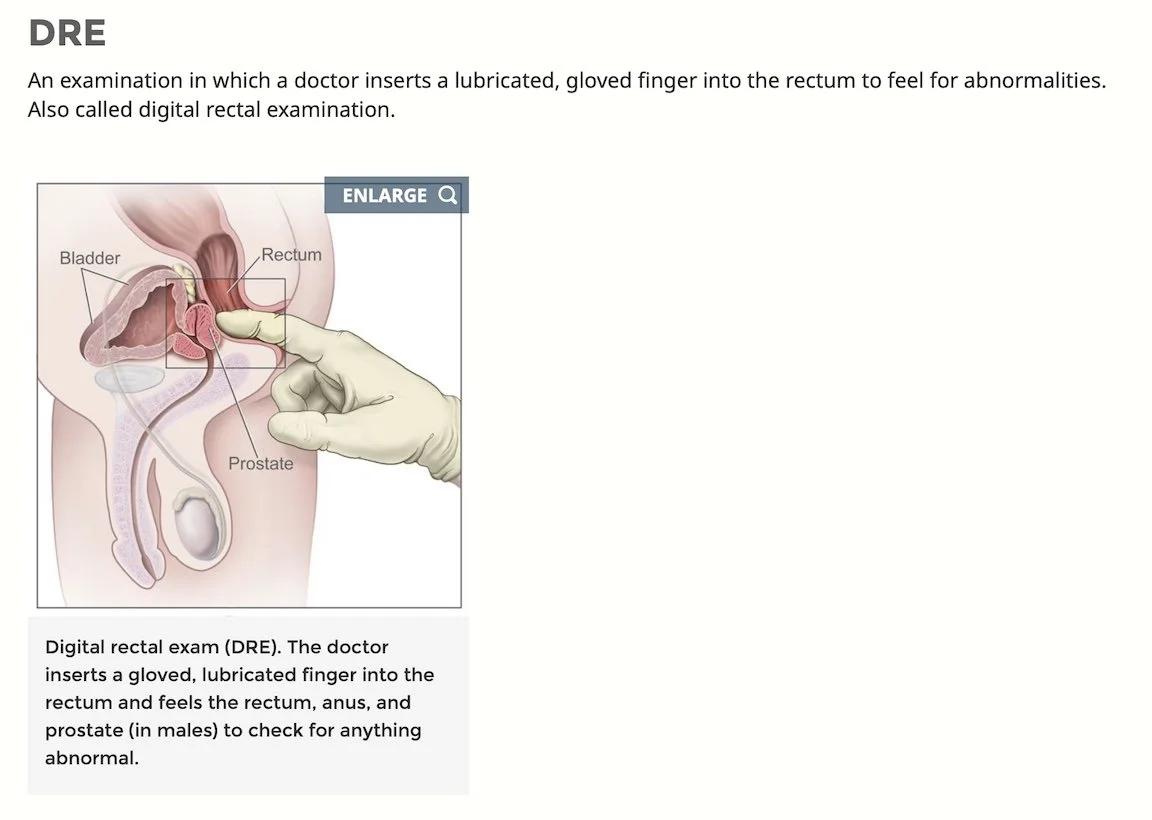
LET'S TOUCH UPON THE PSA, DRE, AND 4-K BLOOD TEST
After eight years of experience with the PSA test, attending countless webinars with medical "experts" and leaders of support groups, here is what I have gleaned from many points of view.
PSA is a check engine light. It's the first in a series of screening tools that can – WITH OTHER SCREENING TOOLS - give you an indication of whether or not you should proceed with further tests – BEFORE considering a biopsy. There are multiple reasons which have nothing to do with prostate cancer for a PSA number to fluctuate or spike. For this reason, the PSA test is never directly linked to a prostate cancer diagnosis. Only a biopsy can do that. Again, and it bears repeating, a high PSA, as a sole check-engine light, does not equal Prostate Cancer. Remember that if anyone suggests otherwise.
Some reasons for a false PSA reading include, but are not limited to the following:
Many men do not know (or are never advised) to refrain from ejaculation for up to 48 hours before having a PSA test, nor do they know to refrain from bike riding or unusual physical exertion for the same period. See this simple review, which provides for other conditions that could affect one's PSA numbers.
Again, while some guidelines call for screening to begin at age 55, other factors could lower that number significantly to age 40 and even before. (When to start screening is a hot oft-debated topic in the PCa world so expect changes). Several conditions can affect the PSA number: family history, genetic testing, ethnicity, and other ailments around your prostate (i.e., enlarged glands, prostatitis, and BPH). Certain medications, as well, can affect the PSA number, and this factor, as well, should be discussed with your doctor(s).
Currently, as of this writing, I have an enlarged prostate of around 80cc. Given this fact, when I monitor my PSA every six months, my doctor and I consider my enlarged gland if I obtain a high PSA reading. The PSA density test then comes in handy, and it is a calculation with which you should be familiar, although, as you will read here, guidelines do not commonly include it in guidelines. Read more here.
THE 4K BLOOD TEST
The 4K test has been a source of confusion for some. Only those who have not been diagnosed with PCa are eligible for this test (if you've had a biopsy, the results would have had to be benign). However, the company that manufactures the test has not conducted the requisite research or trials to have any predictive value for those diagnosed with PCa, even with low risk.
It is an excellent test (and hopefully, your insurance will pay for it) to have as a comparison to your PSA score. Some urologists do not mention this test, so should you be in the position of NOT being diagnosed with PCa and you're just in the middle of a screening process, surprise your doctor and ask for the test if he doesn't suggest it to you. A low score on this test and a low PSA reduce the risk of a false negative result on the latter. Click here for test details and read this STUDY from the NIH, which supports its use as a biomarker.
- From The National Cancer Institute
A urologist usually performs the DRE; however, a primary care physician during an annual physical can do the same. The doc can tell from this exam whether you have an enlarged prostate gland, and they will also be able to know if there could be any abnormal growths. It's another check engine light to accompany the PSA test when considering what, if anything, you may need to investigate further whether you should consider additional testing.
HOLD ON ….THERE’S ANOTHER TEST YOU MAY WANT TO CONSIDER WITH YOUR DR
(Click above for link to MDXHealth)
The National Comprehensive Cancer Network (NCCN) in its latest guidelines, has approved this test as a biomarker which can be used along with blood tests as another check engine light which might lead you to, again, talk to your doctor about additional testing for Prostate Cancer which may include a 3T-MRI and/or prostate biopsy.
Excerpted from the NCCN Guidelines
Download a full PDF of NCCN’s guidelines.
I want to make it clear that the American Urological Association, in its 2022 guidelines, stops short of recommending an MRI before a biopsy (mentioned in earlier blogs only for risk stratification.) It may not preclude a confirming biopsy within the next year, but the disparity in opinions about an MRI following a PSA is unhelpful for the patient. It is why some urologists do not suggest an MRI for men who present rising PSAs. They tend to go straight for a biopsy. I'll add more about this in upcoming blog posts since patients question why doctors recommend an MRI after a patient's biopsy and a possible diagnosis. Or, to put it another way, why couldn't their FIRST procedure be an MRI-guided biopsy?
"Clinical use of the SelectMDx urinary-biomarker test with or without mpMRI in prostate cancer diagnosis: a prospective, multicenter study in biopsy-naïve men." -
Read this May 21 study here.
I've endeavored to lay out a "starter kit," if you will, for what one can do before ever considering having their first biopsy: PSA - DRE - 4K Blood Test - Select DMX. At the time of this writing, I am omitting information about the ExoDx test, as I’m in the midst of researching its efficacy - and use by urologists or specialists - as a biomarker. Stay tuned. These screening tests are essential information to share with friends who have fortunately not been diagnosed with any prostate cancer grade. And, again, work with your doctor. And do your research. You'll be better off succeeding with your shared decision-making process.
—————
Finally, I would like to conclude with my assessment (and my opinion only) of the Prostate Cancer medical community. For certain, there are excellent and competent doctors and specialists across the board, and across this country. Many work tirelessly on behalf of their patients. And there are those, like in many other professions, who may not make the grade insofar as being attuned to the latest studies or guidelines, or may have affiliations with companies - manufacturers of equipment or pharmaceutical companies - which hopefully they disclose. You’ll find them across the board and this country as well, including those who work in locations far away from metropolitan areas or major centers of excellence. Ergo, even though there are guidelines from both the NCCN and AUA (and some of these guidelines, in my opinion, don’t go far enough in keeping up with new developments in the field) doctors will disagree with doctors, or other specialists. It’s the nature of the Prostate Cancer medical community. So, again, as a patient, make sure you’re informed, and that you be discerning when you come upon contradictory information and opinions. As the saying goes:
TRUST BUT VERIFY
I have planned some extra special posts coming up: Healthcare and Health Insurance; (Reminder: the October 15 open enrollment date for Medicare and the ACA (for both Federal assistance and individual state plans) is fast approaching; clearing up questions and confusion about the Transperineal Biopsy; an overview of the nature of support groups; “Your Prostate and Nutrition and Exercise”, and separating out facts from fiction - straight medical news reporting and editorial articles and posts in social media. Healthcare and Insurance play a prominent role in many patients’ lives - I’ll offer a guide to navigating a complex system; many patients who may need to face confirming biopsies or for those following a protocol of having biopsies every 2-5 years have questions with the emerging support for Transperineal biopsies; Support groups are essential to one’s education on Prostate Cancer, and saying that, there are many. You want to be heard, and you want to hear facts. The subject of nutrition, diets, what foods to avoid and what’s best to consume, including supplements, are becoming forefront in discussions, as well as exercise. And let’s discuss “news” vs. “opinions” and, to paraphrase the New York Times: “everything that’s fit to know.”
And, again, I’m a patient, not a doctor nor a scientist. But you can count on me on where and how you can source the best information for your particular situation.
If you haven’t already, please SUBSCRIBE. Simply scroll down to the very end of the blog page to the subscription field in the slightly grey footer section. And feel free to email me with any questions, insights, or even feedback on what I write.
