Hello all. I have been absent from my blog for around three months - but I have a cornucopia of topics to cover while I’ve been on my journey of spinal surgery followed by an unexpected consequence of AUR (acute urinary retention) on which I have several pages to write - about catheterization and my own advocacy around the circumstances which took me there. And, not to, of course, have my physical therapy continue uninterrupted (I’m allowed to be facetious now and then), I’ve been challenged by a new health issue that has had its own difficulties. So, while not out of the woods, I had to notify everyone of a dream come true in the PCa universe where it concerns nutritional and exercise lifestyle,
If you’ve followed me from the beginning of my journey which began with my diagnosis in April 2018 of low-risk PCa for which I’m on Active Surveillance, you would have read that I had taken myself to a health retreat where I embarked on a 3-week program featuring the Hippocrates protocol. Scroll down to my earlier entries and you can re-visit my story about how I adopted a whole food plant-based diet.
Currently, the medical community has not fully embraced the benefits of the WFPB diet; at the most, doctors tout the Mediterranean diet as the heart-healthy diet one can benefit from in all aspects of our health. And, this is true to some extent - many adopt this diet because going off meat, fish, dairy, sugar, etc. is too radical and confining. Understandable. However, anecdotal evidence (which I have encountered) began to rear its head and pointed to this diet as the best in keeping our gut microbiomes clean and buzzing. There are those who have found it to be helpful in bringing their conditions to NED (no evidence of disease) - but, saying that, these cases are NOT documented in scientific and medical journals. Doctors have had very little training in nutrition and it’s hardly their fault that they do not know more on this subject. But, we’ll save that for another day!
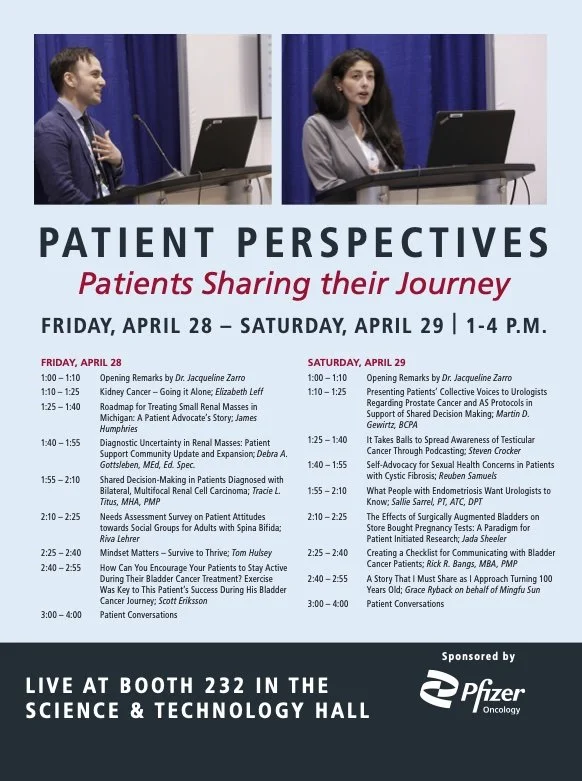
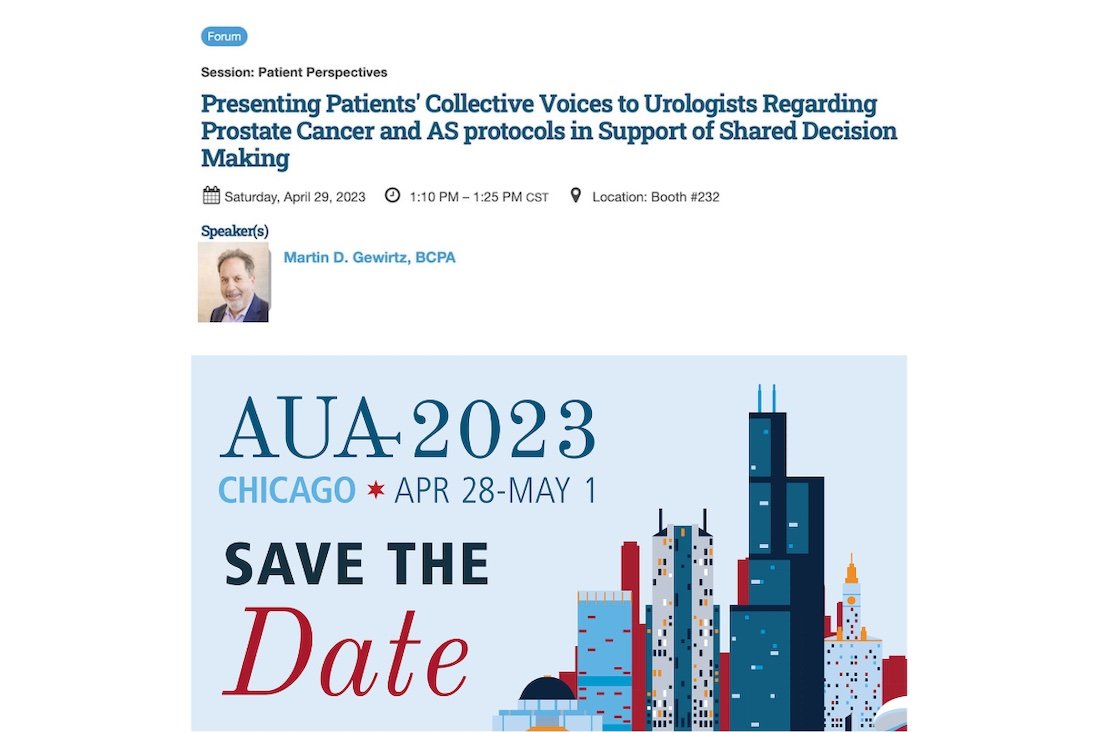
For now, I wanted to bring your attention to a very special FREE webinar being held on Saturday, August, 26th, at 12:00 noon sharp hosted by Active Surveillance Patients International, on which I sit on the Board as a volunteer. Again, at 12:00 Noon SHARP - breaking the glass ceiling (to borrow the cliche) in the latest research (presented at the AUA and ASCO 2023 conferences) on the benefits of whole food plant-based nutritional lifestyle is Stacey Loeb, MD of the NYU Grossman School of Medicine.
ONE CLICK TO REGISTER at https://prostatecancerinfo.org/3E2C3S4
or SCAN the QR CODE below

read more details about Dr. Loeb and what she will be covering
in ASPI’s latest newsletter: https://mailchi.mp/060eabe7dc35/as_101-15591175
AND HERE’S THE BEST PART:
A LIVE Q & A WITH DR. LOEB will follow the presentation!
Everything you need to know will be in these materials. Come with an open mind, or come closed. Come if you’re already on this diet, or if you’re enjoying your summer barbecues. This is a judgment-free zone (and BLOG!).
Finally, my excitement is that this sentiment of embracing a WFPB diet is weaving its way through SCIENCE based research studies and clinical trials. Stay tuned! I’ll follow up with a follow-up - and circle back around again with tales that will benefit you in the long run in how to be your own best advocate. See you Saturday! I’ll be co-moderating with Howard Wolinsky, veteran prostate cancer journalist, AS thriver himself, and the founder of the AS101 series which you can read more about by clicking on links in the ASPI newsletter. Bon Appetite! (Photo above shows just some of the veggies I grabbed at last Saturday’s Farmer’s Market!).